30 year old female with pedal edema and shortness of breath
6-6-2022
Medicine final exam long case
M.Srilekha
I have been given this case to solve in an attempt to understand the topic of patient clinical data analysis to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan.
Chief complaints:
Abdominal pain since 5 days
Facial puffiness and pedal edema since 2 days
Shortness of breath since two days

History of presenting illness:
The patient was apparently asymptomatic 3 months back then she developed facial puffiness and bilateral pedal edema which was pitting type.
Abdominal pain since 5 days which was sudden in onset and of burning type and there are no aggravating and relieving factors.
Later she developed shortness of breath Which was insidious in onset and gradually progressed to grade 4(shortness of breath at rest ) no change on position change and no aggravating and relieving factors.
No history of fever, sore throat ,joint pains.
Past history:
Known case of hypertension since 12 years and on medication.
Known case of chronic renal failure and maintained on dialysis
Total 5 dialysis done in month of may and 4 in June
Not a known case of Asthama, TB, epilepsy, diabetes mellitus, thyroid disorders
No significant past surgical history.
Personal history:
Diet vegetarian
Appetite decreased
Sleep Inadequate
Bowel and bladder regular
No known drug or food allergies
No addictions
Family history:
Mother known case of hypertension.
General examination:
Patient is conscious, coherent and cooperative well oriented to time ,place and person
Pallor present
Icterus absent
Clubbing absent
Cyanosis absent
Generalised lymphadenopathy absent
Edema pitting edema


Vitals
Pulse rate 120bpm
Blood pressure 150/90 mmhg
Respiratory rate 34 cpm
Temperature afebrile
Systemic examination:
Respiratory system:
Patient examined in sitting position
Inspection:
Nose normal
Pharynx normal
Shape of the chest normal
Respiratory movements bilaterally symmetrical reduced
Trachea central in position
Nipples at 4th intercostal
Apex impulse seen at 6th inter coastal space
Palpation:
Trachea central in position
Apical impulse felt ay 6th ics
vocal Fremitus reduced on both sides In infra axillary and infra scapular.
Percussion:
Dull note
Auscultation:
diminished breath sounds on both sides
Cardiovascular system:
JVP not raised
Visible pulsations
Apical pulses shifted downward and laterally to 6th inter coastal space.
Thrills absent
S1 S2 muffled sounds heard
Pericardial rub present
No murmurs
Abdomen examination:
Inspection:
Distended

Umbilicus: normal in position inverted
Movements all quadrants moving normally
Visible pulsations absent
surface of abdomen normal
Palpation:
Liver not palpable
Percussion dull
Auscultation:bowel sounds heard
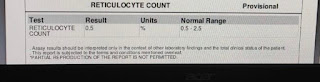
Investigations:













Treatment:








Comments
Post a Comment