40 year old Male with jaundice and pruritus with type 2 diabetes mellitus
This is an online E logbook to discuss our patients' de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through a series of inputs from the available global online community of experts intending to solve those patients' clinical problems with the collective current best evidence-based inputs. This e-log book also reflects my patient-centred online learning portfolio and your valuable inputs on the comment box are welcome.
Name:M.Srilekha(intern)
Chief complaints:
Yellowish discolouration of eyes since 20 days
Itching all over the body since 20 days
History of presenting illness:
Patient was apparently asymptomatic 20 days back then he developed yellowish discolouration of eyes and greenish yellow discolouration of urine
Loss of appetite present
Relieved on medication which was prescribed by local RMP
Loss of weight from 52 kg to 47 kg in 20 days
Abdominal tightness present and relieved on medication
No h/o bloating no h/o abdominal pain, constipation,
Incomplete evacuation of stools since 20 days passing pale coloured stools
No h/o fever, vomiting, diarrhoea
No decrease in urine output
No abdominal distension
Itching all over the body present
History of usage of herbal medication usage for 6 days which aggravated yellowish discolouration and pruritus so stopped using them
Past history:
Past medical history known case of diabetes mellitus since 4 months on Tab.Glimi-M1( METFORMIN 1000mg+GLIMIPRIDE 1mg)
Not a k/c/o HTN CVA CAD epilepsy TB
Past surgical history
No significant past surgical history .
Personal history:
Diet mixed
Appetite decreased relieved on medication
Sleep adequate
Bowel and bladder regular
No known allergies
Habits:regularly takes alcohol 90ml/day stopped 1 month back
Family history: no significant family history
General examination:
Patient is conscious coherent cooperative
Icterus present

No pallor cyanosis clubbing lymphadenopathy edema



Vitals:
PR:80bpm
BP:100/60 mmHg
RR:16 cpm
Spo2:98%
GRBS:238mg/dl
CVS examination:
S1,S2 heard
No additional sounds heard
RS examination: position of trachea central
BAE +, NVBS +
Per abdomen:
Shape of abdomen scaphoid
No tenderness
No palpable mass
Liver palpable:dullness on percussion at 6 th IC space ,lower border 4-5 below costal margin
Liver span 16cpm
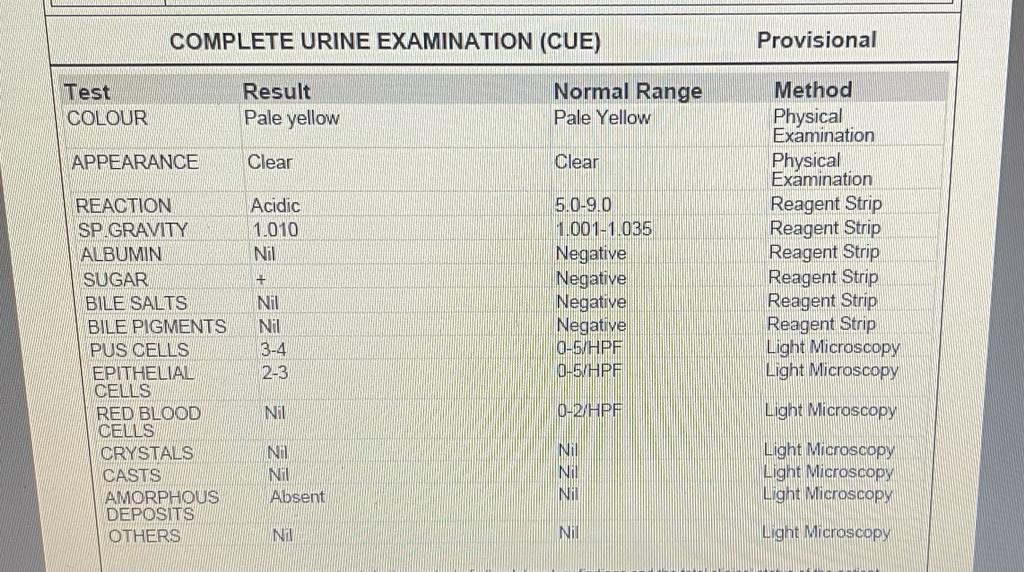
Investigations:
















USG: no sonological abnormality
Chest X-ray:

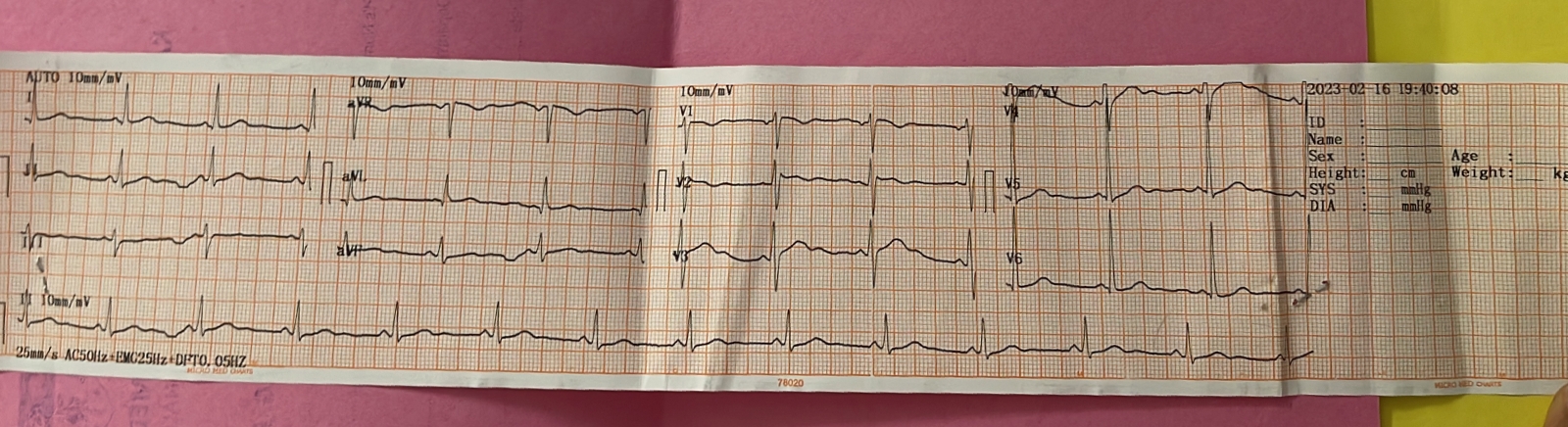
ECG:
2D echo:
Trivial TR, no MR/AR
No RWMA, no AS/MS
Good LV systolic function
No diastolic dysfunction no PAH/PE
Gastroenterologist opinion was taken I/v/o alcoholic liver disease they advised MRCP
Psychiatry referral fine I/v/o alcohol consumption impression:alcohol dependence syndrome currently abstinent
Dermatologist referral I/v/o pruritus
Diagnosis: pruritus secondary to hyperbilirubinemia
Tab. TECZINE 10 mg od/sos
Liquid paraffin/ cebhydra lotion LA/BD
Provisional diagnosis:choleatatic jaundice with pruritus with type 2 DM
Treatment:
Day-1(16/2/23)
1.T.UDILIN 300 mg
2.syp.HEPAMERZ 10 ml po od
3.T.LEVOCET 10mg po h/s 9.00 pm
4.T.GLIMIPERIDE 1 mg po od
5.T.METFORMIN 1000mg po od after breakfast
6.pulse rate , BP , RR, temperature monitoring 4th hourly
Advice at discharge
T.GLIMIPERIDE 1 mg po od
T.METFORMIN 1000mg po od after breakfast
T.HEPTAGON po/bd x1 week
T.BRONAC 60 mg po/ BD x1 week
Cholestyramine oral suspension po/BD x1 week
syp.HEPAMERZ 10 ml po od x 1 week

Comments
Post a Comment